Repeated adjustment of the noninvasive ventilation (NIV) mask to maintain adequate ventilation can contribute to friction and shear on the surface of the skin, and ultimately can lead to pressure injuries.

The utilization of noninvasive ventilation (NIV) for both acute and chronic impaired gas exchange is a common clinical practice. While this type of therapy may help avoid more invasive treatment it is not without consequence.
Noninvasive ventilation has been associated with the development of pressure injuries with rates in the literature ranging anywhere from 10 to 31%.1 A pressure injury is defined as localized damage to the skin and/or underlying soft tissue usually over a bony prominence or related to a medical or other device.6 Human skin is comprised of three layers; the epidermis, the dermis and the hypodermis also referred to as subcutaneous tissue. The significance of a pressure injury is based on the presentation and the depth of the injury within these layers. The depth and/or description of a pressure injury is based on definitions developed by the National Pressure Ulcer Advisory Panel (NPUAP). (See Table 1.) This staging system has been widely used in healthcare since 1989 and have recently been updated.2

Table 1. (Click to enlarge.)
Many factors contribute to the development of a pressure injury and these factors vary from patient to patient. In addition to direct pressure to the skin the presence of moisture and the forces of friction and shear have been linked to the development of a pressure injury.3 A pressure injury associated with NIV is known as a medical device-related pressure injury. The device, specifically the mask interface, creates the pressure which injures the skin. Moisture and heat develop on the surface of the skin between the mask and the skin which alters the skin surface and increases the potential for skin breakdown.4 Repeated adjustment of the NIV mask in order to maintain adequate ventilation can contribute to friction and shear on the surface of the skin. The tolerance of soft tissue for friction and shear forces may also be affected by the patient’s nutritional status, tissue perfusion, the presence of comorbid conditions and the patient’s overall state of health.5
The presence of a pressure injury can cause the patient both physical and emotional pain and it is often associated with increased morbidity and mortality.7 Family members often share the burden of this event as they witness the patient’s discomfort. The failure to prevent the development of a pressure ulcer may result in legal action on the part of the patient.
Additionally, pressure injuries are considered a good indicator of the quality of care that is provided to a patient.6 In 2008, the Centers for Medicare & Medicaid Services (CMS) announced that Medicare will no longer pay the extra cost of treating certain hospital acquired conditions including Stage 3 and Stage 4 pressure injuries.3 Many hospitals are actively looking at ways to reduce the occurrence of pressure injuries, along with other hospital acquired conditions, to meet regulatory requirements.
The greatest risk for a NIV-related pressure injury is during the acute phase of therapy which requires continuous mask application to optimize gas exchange. The injury can occur at any point on the face where any part of the mask meets the surface of the skin. For our ICU’s we most often experienced injury across the nasal bridge. The skin across the nasal bridge is different in that the third layer of skin, is absent, thus the depth from skin surface to bone is minimal and the risk for rapid injury evolution is significant.2
The clinical goal of NIV utilization should be both stabilization of gas exchange with the prevention of a pressure injury.7 Preventing pressure injuries associated with NIV can be a daunting task because the population of patients that require NIV. Our patients often present with multicomorbidities including one or more chronic diseases, medical frailty, and poor nutritional intake. Long-term steroid use is a common factor is also common in our patient population. Together these factors increase the risk for pressure injury development secondary to making the skin more fragile and prone to injury.5
Introduction
At our institution we noticed a significant increase in the number of pressure injuries associated with NIV from one fiscal year to the next (24 occurrences in FY16). To address this problem, a multidisciplinary team was formed with the goal of developing a plan to reduce the incidence of pressure injuries.
The team was comprised of the following disciplines: providers who manage the patients who require NIV, critical care nurses including a member of the hospital’s wound team, respiratory therapists whom manage NIV therapy and clinical educators from both nursing and respiratory. Together we performed a collaborative assessment of our current noninvasive ventilation practices.
Methods
The first step was to evaluate the current mask that was used for NIV. When evaluating other mask options we recognized the inherent limitations in mask design in that any mask designed for noninvasive ventilation would require continuous pressure against the skin. After looking all of our options the team chose an oral-nasal mask that allowed for smoother placement on and off the patient’s face. The respiratory therapists received individualized, hands-on education regarding proper fit of the mask.
For patients who required NIV for longer than six hours we alternated the use of a full-face mask with an oral/nasal mask in order to help redistribute the pressure across the skin surface of the face. This option was patient dependent as some patients could not tolerate the application of a full-face mask. The respiratory therapist would be responsible to manage the schedule of mask rotation which would occur every four to six hours depending on the patient’s clinical condition. Both the nurse and the respiratory therapist would be responsible to evaluate the skin surface when the mask is removed. The prevention of pressure injury is a complex process and requires constant vigilance to achieve success.6
Next, in conjunction with our skin expert, we looked at the skin barrier products that were available for use. We had experienced short-term success a few years ago when we began using a lightweight foam dressing between the rim of the mask and the skin surface. However, the success was short-lived.
In the end we chose a gel-type of barrier which would be placed between the rim of the mask and the surface of the face. The barrier we chose offered the option of an individualized fit as it could be cut to fit each patient’s facial features. The gel barrier would be applied to all NIV patients at start of therapy.
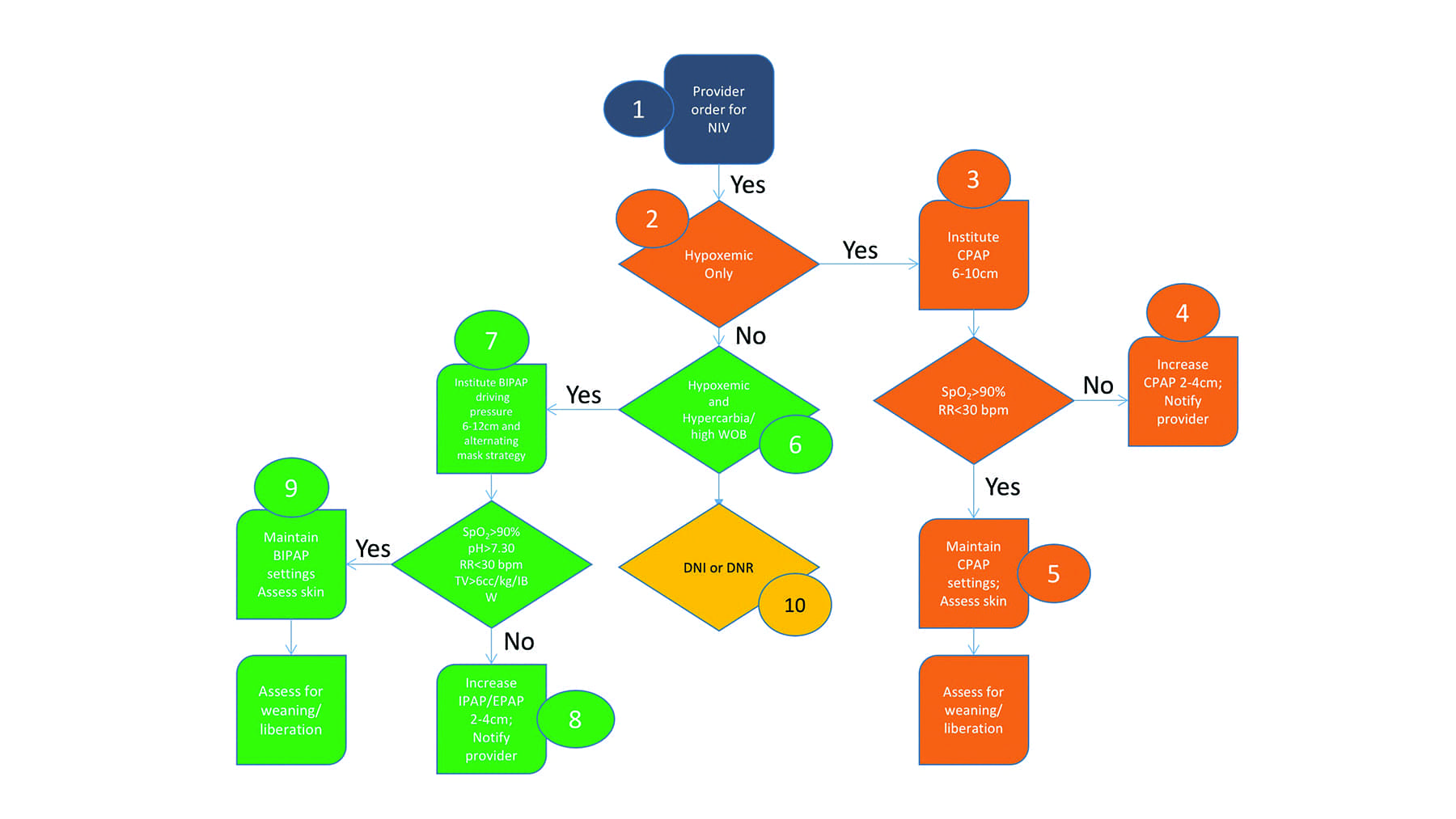
Figure 2. NIV Protocol. (Click to enlarge.)
Perhaps the most important step in this process was the development of a NIV algorithmic protocol. (See Figure 2.) We evaluated our clinical practice to assure that use of noninvasive ventilation was appropriate for the patient and that we were consistent in our practice. Developing an algorithmic protocol allowed us to guide the use of NIV across the network. Once the algorithm was developed we created an order set to match the algorithm. The new order set requires the provider to define specific clinical endpoints when placing the order for NIV. These clinical endpoints included the following: target SpO2 level, a maximum allowable respiratory and heart rate, and arterial pH and NIV liberation endpoints. (See Figure 3.)

Figure 3. Defined Clinical Endpoints. (Click to enlarge.)
These defined endpoints contributed to more appropriate NIV parameter adjustments with the end result of improvement in the overall clinical management of NIV. Daily rounding on the NIV patient population was conducted to ensure adherence to the algorithm and also provided opportunities for additional NIV education as needed.
After a trial period in the ICU the algorithm was moved other critical care units within the hospital. We followed the same process when providing education for all levels of caregivers who interact with patients who require NIV. Once again the education included correct mask sizing, mask application and removal techniques, review of the clinical management and specific clinical end-points for NIV failure and success, liberation criteria, and the roles and responsibilities of all the NIV team members.
Data Collection & Analysis
Frontline clinicians who assessed for and recognized the presence of a pressure injury caused by NIV completed an electronic patient safety report (PSR). Data was collated on patient population, device used, and injury location. The pre-intervention, intervention, and post-intervention unit level data was analyzed monthly on the number of NIV pressure injury events.
Results & Discussion
In FY16 we reported 24 pressure injuries hospital-wide related to mask use during noninvasive ventilation. In FY17 the total number of NIV device related pressure injuries dropped to five, a a 79% reduction. (See Figure 4.)
What contributed most to our successful reduction in the occurrence of pressure injures? We knew from the start that there wasn’t going to be a single action/intervention that would reduce our pressure injury rate. We approached the problem with three main goals; to find a mask with a better fit, to look for a more effective skin barrier and to critically evaluate how we provide noninvasive ventilation therapy to our patients.

Table 4. Number of NIV Device-related Pressure Injuries. (Click to enlarge.)
We strongly believe that involving all disciplines of care providers in the design of the protocol/algorithm was vital to its success. Each member of the team was able to contribute his or her expertise to improve the care of the patient receiving noninvasive ventilation. Thus all team members were engaged to achieve a successful outcome. Education of all members of the care team was imperative as it facilitated communication among the care team in the day to day management of the patient.
Also, the development of specific NIV endpoints in terms of desired clinical outcomes was very beneficial. The endpoints became goals, which, when met, would result in successful therapy for the patient. Future endeavors in this process include looking at the duration of noninvasive ventilation and its impact on ICU length of stay.
Conclusions
A pressure injury can be an undesirable side effect of NIV clinical management. All attempts should be made to minimize the occurrence of a pressure injury while the patient is receiving noninvasive ventilation. Based on our strategic process we were able to reduce the occurrence of pressure injuries significantly. As a result we advocate the implementation of a multidisciplinary team to assess and evaluate current NIV practices and develop a strategic process to maximize patient outcomes and minimize pressure injuries. RT
Kenneth Miller, MSRT, MEd, RRT-ACCS, FAARC, Lucy Cascioli, MSN, RN, ACNS-BC, Christine Harter, MSN, RN, and Munawer Kermalli, MBA, MHA, are clinicians at Lehigh Valley Health Network, Allentown, Pa. For more information, contact [email protected].
References
- Schallom, Marilyn et al. 2015. Pressure Ulcer Incidence in Patients Wearing Nasal-Oral Versus Full-Face Noninvasive Ventilation. American Journal of Critical Care. 24(4): 349-357
- Black et al. 2017. National Pressure Ulcer Advisory Panel’s Updated Pressure Ulcer Staging System. Advances in Skin & Wound Care 20 (3): 269-274.
- Cooper, K. 2013. Evidence-Based Prevention of Pressure Injuries in the Intensive Care Unit. Critical Care Nurse. 33(6): 57-66.
- Black et al. 2010. Medical Device Related Pressure Ulcers in Hospitalized Patients. International Wound Journal. 7(5):358-365
- Edsberg et al. Unavoidable Pressure Injury: State of the Science and Consensus Outcomes Journal of Wound Ostomy & Continence Nursing.August 2016: 41(4):313-321.
- Lyder, C. 2003. Pressure Ulcer Prevention and Management. Journal of the American Medical Association. 289 (2). pp 223-226.
- Ratliff et al. 2017. WOCN 2016 Guideline for Prevention and Management of Pressure Injuries. Journal of Wound Ostomy and Continence Nursing. 241-246.
- Stacy, K. (2104). Pulmonary Therapeutic Management [Unit lll Pulmonary Alterations]. In L. Urden, K. Stacy, & M. Lough (Authors), Critical Care Nursing, Diagnosis and Management, (Vol. 7, pp.571-573). St Louis, MO: Elsevier.