Pulse oximetry is a standard diagnostic for detecting critical congenital heart defects (CCHD) in newborns. However, there is variation in which algorithms and methods clinicians use to test neonates.
By Rose Rimler

In 2010, the Department of Health and Human Services (HHS) added critical congenital heart defects, or CCHD, to the list of conditions that it suggests all newborn babies be screened for. Cardiovascular abnormalities account for more infant deaths than any other birth defect, and CCHD includes some of the most serious diagnoses, affecting an estimated two infants per 1000 live births.1-2
Shortly after the HHS endorsement, a federally-appointed committee gave providers some guidelines on how to enact the screening. The guidelines rely on a common, relatively inexpensive piece of equipment called a pulse oximeter, which uses light to measure the oxygen content of blood through a newborn’s foot or hand.
States soon began heeding the federal government’s advice. In 2011, New Jersey became the first state to require routine pulse oximetry screening (POS) of newborns; now every state in the union and the District of Colombia has adopted or is in the process of adopting some version of the screening, mandatory or not.3 But not all states follow the algorithm set out by the 2011 committee, and that algorithm varies from what other countries endorse. So which algorithm is best?

Gerard Martin
That’s what Andrew Ewer and Gerard Martin set out to investigate in a Pediatrics paper4 published in November. Martin, a cardiologist at Children’s National Health System, was an author of the US recommendations. Ewer, a professor of neonatal medicine at Birmingham Women’s Hospital in England, led the pulse ox study5 that helped inform the panel.
“When we made the US recommendations, the number one worry amongst pediatric cardiologists was that we might create a lot of unnecessary work for [them,]” Martin said. “In other words, there was a lot of concern about false positive tests. So when we chose an algorithm for the US we opted to adjust the algorithm so that we would minimize the false positives without trying to compromise on the true positives.”
To walk that fine line, Martin and colleagues came up with a protocol that recommends testing of the right hand and one foot; performing the test when the baby is between 24 and 48 hours old; and retesting twice if oxygen saturation is less than 95% or if the difference in saturation between the foot and the hand is greater than 4%. (See Figure 1.)
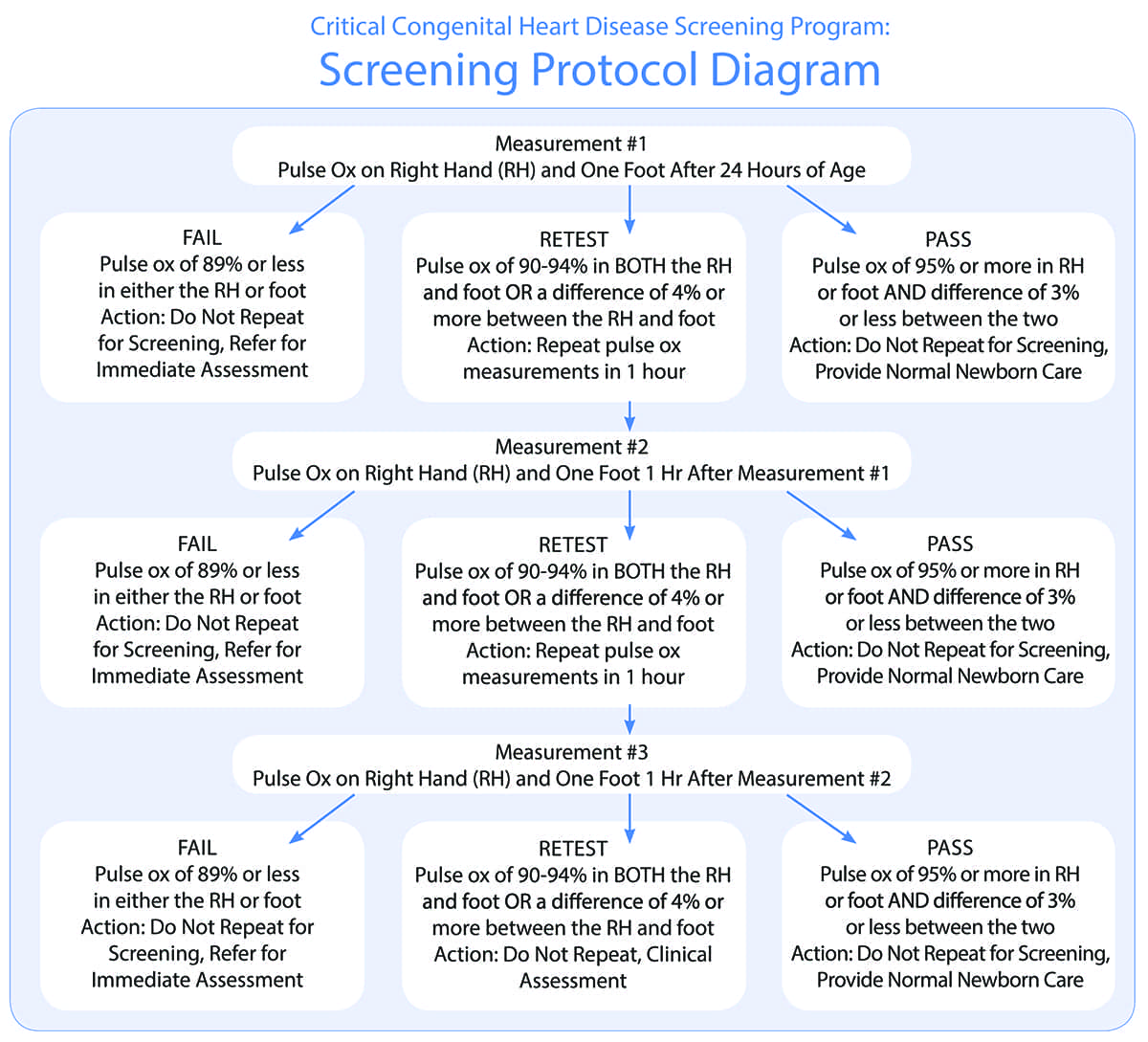
It was an intentionally conservative approach, meant to recognize the heterogeneity of medical care in this country. Not all American babies are born in hospitals with easy access to pediatric cardiologists. “There was a lot of concern that we would be moving babies between hospitals, separating them from their parents to get tests that were unnecessary,” Martin said.
But that concern has turned out to be unfounded, Martin said. While not every baby who tests positive for CCHD has a heart defect, many have something else that the pediatrician needs to know about, such as pneumonia, sepsis, or pulmonary hypertension. Somewhere between 30 and 80% of these “false” positives result in such a diagnosis, which can usually be determined by a generalist, Martin said.

“If you’re getting what we would consider a false positive and then you find a severe pneumonia or genetic lung abnormality, clearly [the screening] has accomplished its goal,” said Aaron Dorfman, a cardiologist at Children’s Hospital of Philadelphia who was not involved with the study. After all, he explained, the goal is to catch serious disease before the baby leaves the hospital.

Andrew Ewer
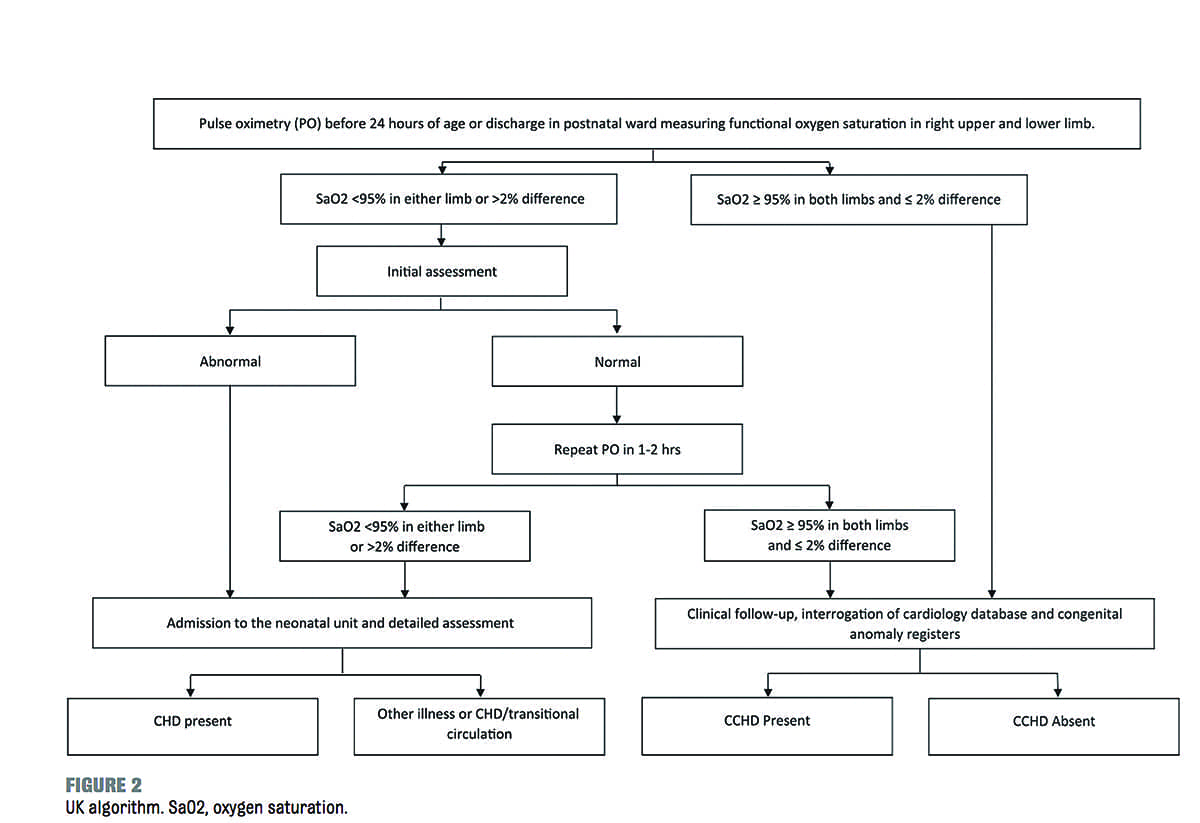
If many false positives are beneficial, then perhaps the algorithm should be adjusted to a less conservative approach, Martin and Ewer write. One option would be the algorithm Ewer proposed in his pulse ox study. Unlike the US recommendations, Ewer’s protocol calls for testing when the baby is less than 24 hours old and suggests one re-test in an otherwise healthy baby if oxygen saturation is less than 95% or if the difference in saturation between limbs is greater than 2%. (See Figure 2.) When Ewer applied the US protocol to the raw data in the pulse ox study, which examined about 20,000 newborns, he found that one patient with CCHD and two patients with CHD would have been missed.
 Those numbers might add up when applied to the total US birth rate of four million per year, Ewer noted.6 Still, neither author suggests that there is enough evidence to call for a widescale change from the US to the UK protocol. (Ewer and others are lobbying the British government to adopt the screening measures proposed in the Pulse Ox study.) What is most convincing, they conclude, is evidence in favor of shifting the timing of the test up to the first day of an infant’s life to ensure detection before symptoms present, despite the inevitable increase in false positives.
Those numbers might add up when applied to the total US birth rate of four million per year, Ewer noted.6 Still, neither author suggests that there is enough evidence to call for a widescale change from the US to the UK protocol. (Ewer and others are lobbying the British government to adopt the screening measures proposed in the Pulse Ox study.) What is most convincing, they conclude, is evidence in favor of shifting the timing of the test up to the first day of an infant’s life to ensure detection before symptoms present, despite the inevitable increase in false positives.
Dorfman, who practices in New Jersey, supports the screening procedure in place and recalls some “memorable” patients whose CCHD was detected by the routine POS New Jersey instated in 2011. But he’s hesitant about a revision that would result in a safety net with a tighter weave.
“Already our health care costs are very high. By adding expensive testing such as echocardiography it could add to the overall health care cost burden,” Dorfman said. Plus, he added, there’s the hard-to-quantify cost of unduly stressing out new parents, and the added burden on cardiologists.
“If you talk about doubling or tripling the number of babies that need to be evaluated, we’re talking about needing additional resources.”
Since the federal guidelines are suggestions rather than law, states are free to implement their own protocols, which can be less strict. In Tenessee, for example, providers are told to first test the foot alone.7 That makes for a lighter workload, but increases the chance that babies with certain conditions might be missed, Martin said. As rare as those, and CCHD in general, may be, undiagnosed critical heart defects are devastating to families who bring home an apparently healthy baby who suddenly stops breathing.8 In general, parents are advocates in favor of screening, Martin said.
As for time and expense, the initial testing is thought to cost less than 10 dollars and 10 minutes of a provider’s time.9 The expense goes up significantly if a baby is referred for an echocardiogram, as Dorfman pointed out.
Alex Kemper, a professor of pediatrics at Duke University and deputy editor of Pediatrics, is open to the idea of an altered POS algorithm, even if it flags more babies who turn out okay. “Babies should not have low levels of oxygen in their blood,” he said. “The clinicians that take care of babies know how to work up and evaluate babies who have low levels of oxygen in their blood. In some cases it might mean that a baby needs to be transferred for something like an echocardiogram, but those referral systems are already in place across the country.”
What about other parts of the world? Both Ewer and Martin are advocates for implementing POS worldwide, even in developing countries where families may not have access to the health care necessary to treat babies with heart defects. For one, the screening might catch other, more easily treated, conditions. But it’s also a question of fairness, Martin said.
“Shouldn’t every mother know that something’s wrong with her child before they leave their birth facility?”
In the US, Martin has noticed a “paradigm change” in the few short years since screening has been implemented. Now, when a baby is admitted into the ICU with CCHD, staff demand to know why the condition wasn’t caught sooner.
“It used to be that everyone accepted that there were going to be late diagnoses,” he said; now, the cardiac ICU experts at his hospital expect CCHD to be found before a baby shows symptoms.
With POS added to antenatal screening and visual examination of newborns, Ewer estimates the success rate of finding these babies will go up to 95%. As for finding the right algorithm, it’s an “evolving” process, he said. “The tighter the cutoff, the more likely you are to pick up more defects. It’s that balance of what are people willing to accept. How many babies is it ok to miss and how many babies is it ok to test positive?” he said. “It’s up to individual societies to think about.” RT
Rose Rimler is associate editor of RT. For further information, contact RTmagazine@allied
360.com
References
- “Facts About Critical Congenital Heart Defects.” Date Accessed 12/23/16. https://www.cdc.gov/ncbddd/heartdefects/cchd-facts.html
- Glidewell, J. et al., “State Legislation, Regulations, and Hospital Guidelines for Newborn Screening for Critical Congenital Heart Defects — United States, 2011–2014.” Morbidity and Mortality Weekly Report. 2015; 64(23);625-630 https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6423a1.htm?s_cid=mm6423a1_w
- “Newborn Screening Map: All Disorders.” Date Accessed 12/23/16. https://www.newsteps.org/newborn-screening-status-map-all-disorders
- Ewer, AK and Martin, GR. “Newborn Pulse Oximetry Screening: Which Algorithm Is Best?” Pediatrics. 2016; 138 (5); e20161206 http://pediatrics.aappublications.org/content/138/5/e20161206?sso=1&sso_redirect_count=3&nfstatus=401&nftoken=00000000-0000-0000-0000-000000000000&nfstatusdescription=ERROR%3A No local token&nfstatus=401&nftoken=00000000-0000-0000-0000-00000
- Ewer, AK et al., “Pulse oximetry screening for congenital heart defects in newborn infants (PulseOx): a test accuracy study.” The Lancet. 2011; 378 (9793) 785-794. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(11)60753-8/abstract
- “Births and Natality.” Centers for Disease Control National Center for Health Statistics. Date Accessed: 12/23/16. https://www.cdc.gov/nchs/fastats/births.htm
- “Protocol for Critical Congenital Heart Disease (CCHD) Screening.” Tennessee Department of Health. Date Accessed 12/23/16. https://tn.gov/assets/entities/health/attachments/CCHD_Screening_Protocol_Algorithm.pdf
- Berger, Susan. 4/7/2014. “Saving Babies: An Inexpensive, Easy Oxygen Test Can Prevent Many Deaths.” The Washington Post. https://www.washingtonpost.com/national/health-science/saving-babies-an-inexpensive-easy-oxygen-test-can-prevent-many-deaths/2014/04/07/3c6c8b2a-9b12-11e3-975d-107dfef7b668_story.html?utm_term=.c1aaa00b47ff
- Ewer, AK et al., “Pulse oximetry as a screening test for congenital heart defects in newborn infants: a test accuracy study with evaluation of acceptability and cost-effectiveness.” Health Technology Assessment. 2012; 16(2) 1-184. https://www.ncbi.nlm.nih.gov/pubmed/22284744







